Is it time to
work on you?
Melbourne counselling, hypnotherapy, psychotherapy and psychology




You’ve already done the hard part.
Deciding you want to change takes real courage and honesty. And you did that alone. For the rest, you have access to counselling and psychotherapy support in Melbourne and online.
At Bayside Psychotherapy, we strive to help you make the changes you want to make in your life and make those changes stick.
Together, we may be able to unearth deeply ingrained inner conflicts to make you feel genuinely better. Not in a ‘Gosh I’m glad I’m helping myself’ kind of way, but in a ‘This is how life is supposed to feel!’ kind of way.
Counselling & psychotherapy

Hypnotherapy & NLP therapy

Couples counselling

Online & in-clinic therapy

Our Therapists

Adam Szmerling
Psychoanalytic Psychotherapist

Kelli Tranter
Hypnotherapist & Counsellor

Lawrence Akers
Clinical Hypnotherapist & Counsellor

Natalie Szmerling
Clinical Psychologist

Carolina Rosa
Counsellor and Hypnotherapist

Sara Herring
Hypnotherapist and Counsellor

Humaira Ansari
Hypnotherapist & NLP Therapist
Why Choose Us?
Frequently Asked Questions
What is a psychotherapist?
A psychotherapist is a professional who takes a depth approach to working with a persons suffering, rather than by means of medical intervention or working on surface symptoms. They work to collaborate with individuals in order to observe their attitudes, conflicts, and behaviours that form the current quality of that person’s life, relationships, and social status. Their work often goes much deeper to uncover the root causes of problems, which may result in a more dramatic change in perspective to the patient. Ultimately, psychotherapists aim to treat their patients by empowering them to break free of their unconscious triggers or impulses through increased self-awareness, though the process can be longer than counselling.
Do you work with NDIS funded clients?
Yes, but at this stage, only Kelli Tranter, Carolina Rosa and our Social Worker & Psychoanalytic Psychotherapist Adam Szmerling works with adult clients who are either Self-Managed or Plan-Managed through their NDIS therapeutic services provider. Please call reception on 9557 9113 or email us to discuss your requirements and make a booking. Please do not book online for NDIS sessions.
What training, qualifications and experience should Australian counsellors and psychotherapists have?
A formal qualification is not currently required to work as a counsellor in Australia, but highly recommended for best practice. Australian counsellors and psychotherapists commonly hold a minimum of an undergraduate degree in a health-specific area, plus additional training in psychotherapy, which may typically take three to four years of education to obtain. Additionally, some counsellors and psychotherapists are required to undergo a period of personal psychotherapy to ensure they have suitable levels of self-awareness to be able to support and treat patients. As well as holding a university degree, Australian counsellors and psychotherapists will have extensive experience working across a multitude of conditions and may hold professional memberships with the Psychotherapy and Counselling Federation of Australia.
How regularly will I see my counsellor or psychotherapist?
It depends on the therapist and their suggestions and methods of practice, however, we believe that lasting change and deep improvements in self-esteem stem from frequent, consistent visits.
On average, patients will see their counsellor or psychotherapist weekly, whilst some patients choose to attend fortnightly, others may choose to visit more or less frequently than that. For depth psychotherapy more than once a week over several months or years is common as people become more curious about how they tick and want to probe deeper. Once in session, your therapist will discuss your recommended visit frequency with you, and working together you will both choose a suggested frequency of visit that suits your unique circumstances. They will take into account your current situation, lifestyle, and availability. This will be collaborative.

Choosing the right therapist: The 5 most important considerations
Choosing the right therapist can be difficult. Different problems and different personalities call f...
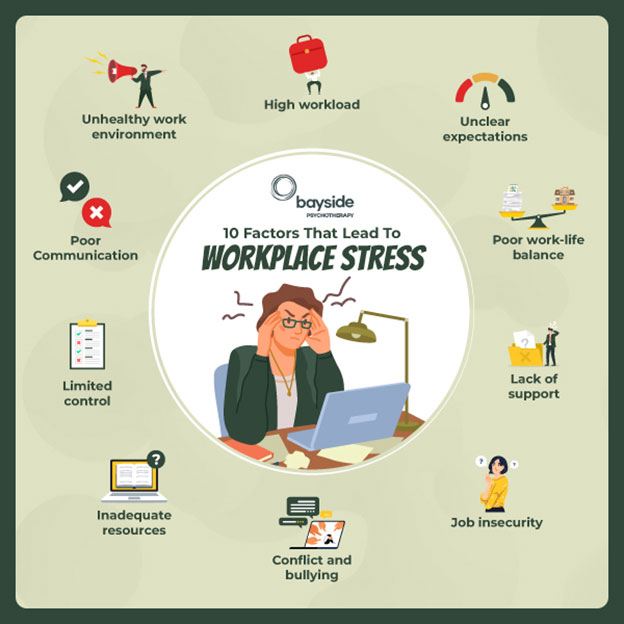
Creating Healthier Workspaces: How stress leave can foster happier, healthier, and more productive employees
Employee mental health is pivotal to overall workplace wellbeing, impacting individual performance, job satisfaction, and organisational productivity. Th...

From High Stakes to Healing: 8 Tips To Overcome Gambling Addiction
Gambling activities have become more accessible and convenient due to the proliferation of casinos and the rapid growth of online gambling platforms. Moreover, technological adva...
Email Us
Call us
Reception Phone Hours
- – Monday 8:30am to 5:30pm
- – Tuesday 8:30am to 5:30pm
- – Wednesday 8:30am to 5:30pm
- – Thursday 8:30am to 5:30pm
- – Friday 8:30am to 5:30pm
Closed on public holidays
Choose your own date and time for an online or in-clinic session
Therapist Hours
- – Monday 8:00am to 8:00pm
- – Tuesday 8:30am to 8:00pm
- – Wednesday 8:30am to 8:00pm
- – Thursday 8:30am to 8:00pm
- – Friday 8:30am to 8:00pm
- – Saturday 8:00am to 6:00pm
Closed on public holidays

